")
Topography, contour, size, distribution and margins
These viral infectious areas or mildly neoplastic changes are usually adjacent to the squamocolumnar junction (SCJ) and engulfed in areas of immature metaplasia, but they can be found anywhere in the transformation zone (TZ) or outside it on the squamous epithelium of the ectocervix or even in the endocervical canal. One of the greatest challenges in colposcopy is accurately diagnosing CIN1, particularly in young women in whom an abundance of immature portions of the cervical transformation zone are visible (figure 49).
The distribution of LSILs varies from unifocal to multifocal. Multiple, distinct, small, randomly scattered lesions are characteristic of LSILs. These may be located within or outside of the transformation zone (figure 50). It is not uncommon to see coexisting HPV-related disease extending into the vagina in the form of condyloma or vaginal intraepithelial neoplasia.
The majority of CIN1 lesions are macular in contour. In some cases it may be maculopapular. LSILs generally represent an acute epithelial HPV infection and usually they tend to be diffuse and asymmetrical in shape. They usually have irregular borders and their margins vary tremendously, assuming geographic, feathered, flocculated, or indistinct demarcations from surrounding normal epithelium (figures 51, 52).
Condylomas may present on the cervix as exophytic condylomata acuminata or as flat to slightly raised satellite lesions. These may be found inside or beyond the TZ. Condylomatous lesions may vary in surface contour, from flat acetowhite lesions to slightly raised areas with regular fine papilla to florid exophytic condylomata acuminata. Flat acetowhite macular lesions are sometimes referred to as flat condylomata (figure 50).
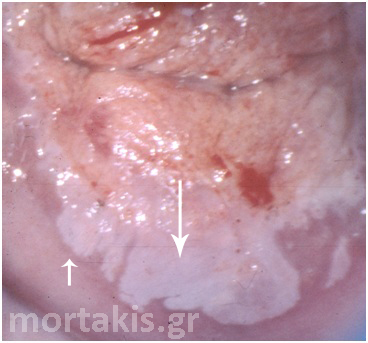
Figure 49 Transformation zone and SQJ are seen. Biopsies showed immature squamous metaplasia (small arrow) and CIN1 (large arrow). In almost half of similar cases, colposcopists cannot differentiale accurately between ISM and LSIL.

Figure 50 LSIL on the mature squamous epithelium of the ectocervix (flat condylomata) as well as in the transformation zone.
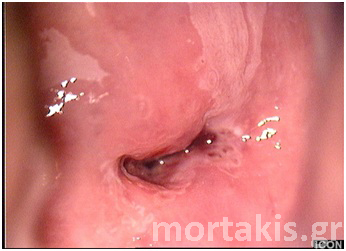
Figure 51 “Satellite” LSIL lesion on the left upper part of the picture and immature metaplasia (ISM) on the right upper part. Biopsy at 3 o’clock showed CIN1.
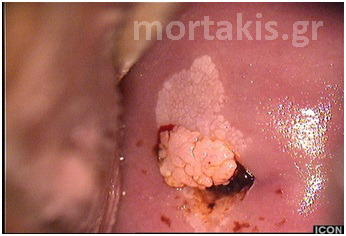
Figure 52 LSIL lesions of the cervix. CIN1 at the anterior lip and exophytic condyloma acuminatum protruding from the cervical os.
Color
Prior to the application of the 5% acetic acid, most CIN1 lesions have a normal pink epithelial color. After the application of the 5% acetic acid some lesions appear almost translucent white or faint white, but generally not as translucent as immature metaplasia (figure 53).
The acetowhite effect on CIN1 lesions is more gradual in onset and more transient in duration than the acetowhite reaction seen in higher-grade dysplasia. In addition, the dilute acetic acid needs to be reapplied frequently for optimal visualization of the lesion. 
Figure 53 Typical acetowhiteness of a CIN1 lesion
Cervical condylomas may be shiny white, conveying an opaque quality. Because of the keratin, some condylomas also appear white prior to the application of 5% acetic acid solution (figures 54, 55).

Figure 54 Shiny white condylomatous lesion of the cervix

Figure 55 White cervical condylomas at the upper cervical lip, with elevated, micropapillary surface.
Vessels
Low grade squamous lesions may exhibit vascular changes including punctation and mosaic but the blood vessels usually have a fine, narrow caliber. A slightly increased intercapillary distance may be seen, but the vessel spacing is usually similar to that in normal tissue (figures 20, 38).
The vessels of CIN1 are arranged uniformly. Consequently, a mosaic vascular pattern associated with CIN1 is homogeneous in distribution and appears homogenous in distribution. Punctation is observed as tiny red dots closely and uniformly distributed (figure 56).
Each papilla of an exophytic condyloma acuminata has a central capillary loop that may be most easily seen after the dilute acetic acid has begun to fade (figures 57, 58).
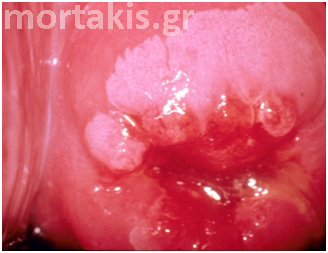
Figure 56 Usual vascular patterns of immature squamous metaplasia and LSILs.

Figure 57 Vascular patterns of cervical condylomata acuminata. “Loop vessels” of condylomata may be confused with atypical vessels.

Figure 58 Cervical condylomata of the figure 57 after the application of acetic acid solution.
Iodine staining
CIN1 lesions are iodine negative with a mustard yellow color after the application of dilute Lugol’s iodine in areas that were formerly acetowhite. Because CIN1 is frequently positioned in a field of immature metaplasia, both areas will appear yellow following application of Lugol’s iodine solution, and thus may blend together, making differentiation challenging (figure 59).
Occasionally, there may be a variegated yellow and brown pattern noticed in focal epithelium that contains variable amounts of glycogen. Because glycogen is usually found in intermediate and superficial layers of squamous epithelium and the atypical cellular changes of CIN1 are found primarily in the basal and parabasal layers, it is not uncommon to see some degree of partial or even full iodine uptake in isolated areas of CIN1(figure 60 a & b).


Figure 59 (a & b) Partial iodine uptake by immature squamous metaplasia and CIN1.
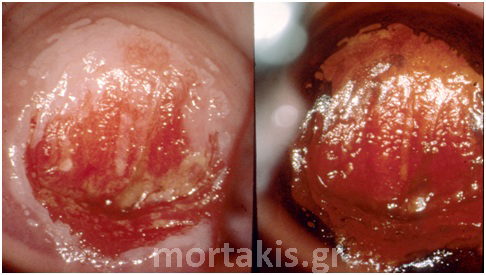
Figure 60 (a & b) CIN1 lesions on the left part of the picture, immature squamous metaplasia on the right. A) after acetic acid solution, and b) after application of Lugol’s solution.
